Endometriosis Treatment in Chennai
From accurate staging to fertility-preserving surgery and IVF — a targeted approach to managing endometriosis and helping you conceive.

Endometriosis is one of the most underdiagnosed conditions in reproductive medicine, with many women waiting years before receiving a correct diagnosis. The condition occurs when tissue similar to the uterine lining grows outside the uterus — on the ovaries, fallopian tubes, pelvic peritoneum, and sometimes beyond — causing chronic inflammation, pain, and scarring that can significantly impair fertility. At our Chennai clinic, Dr. Rukkayal combines advanced diagnostic methods with both surgical and reproductive treatment options to provide comprehensive care.
Endometriosis management demands a balance between symptom relief and fertility preservation. Dr. Rukkayal's approach begins with precise staging — determining whether you have minimal, mild, moderate, or severe disease — because treatment decisions differ substantially at each level. For women seeking pregnancy, the strategy may involve laparoscopic excision of endometriotic lesions to restore pelvic anatomy, followed by a defined window for natural conception or assisted reproduction. When IVF is the most appropriate path, Dr. Rukkayal's direct involvement in the embryology laboratory ensures that egg quality, fertilization, and embryo development are managed with the heightened attention that endometriosis patients require, as the condition can affect oocyte and embryo quality even when tubes remain open. Every treatment plan is individualized, accounting for your symptom severity, extent of disease, ovarian reserve, age, and personal fertility timeline.

500+
Endometriosis Surgeries
60-70%
Post-Surgery Conception Rate
Symptoms That May Indicate Endometriosis
You should see a specialist if you experience:
- Progressively worsening painful periods (dysmenorrhea)
- Pain during or after sexual intercourse (dyspareunia)
- Chronic pelvic pain that persists outside of menstruation
- Difficulty conceiving despite regular cycles
- Painful bowel movements or urination during periods
- Heavy menstrual bleeding or spotting between periods
Understanding Endometriosis
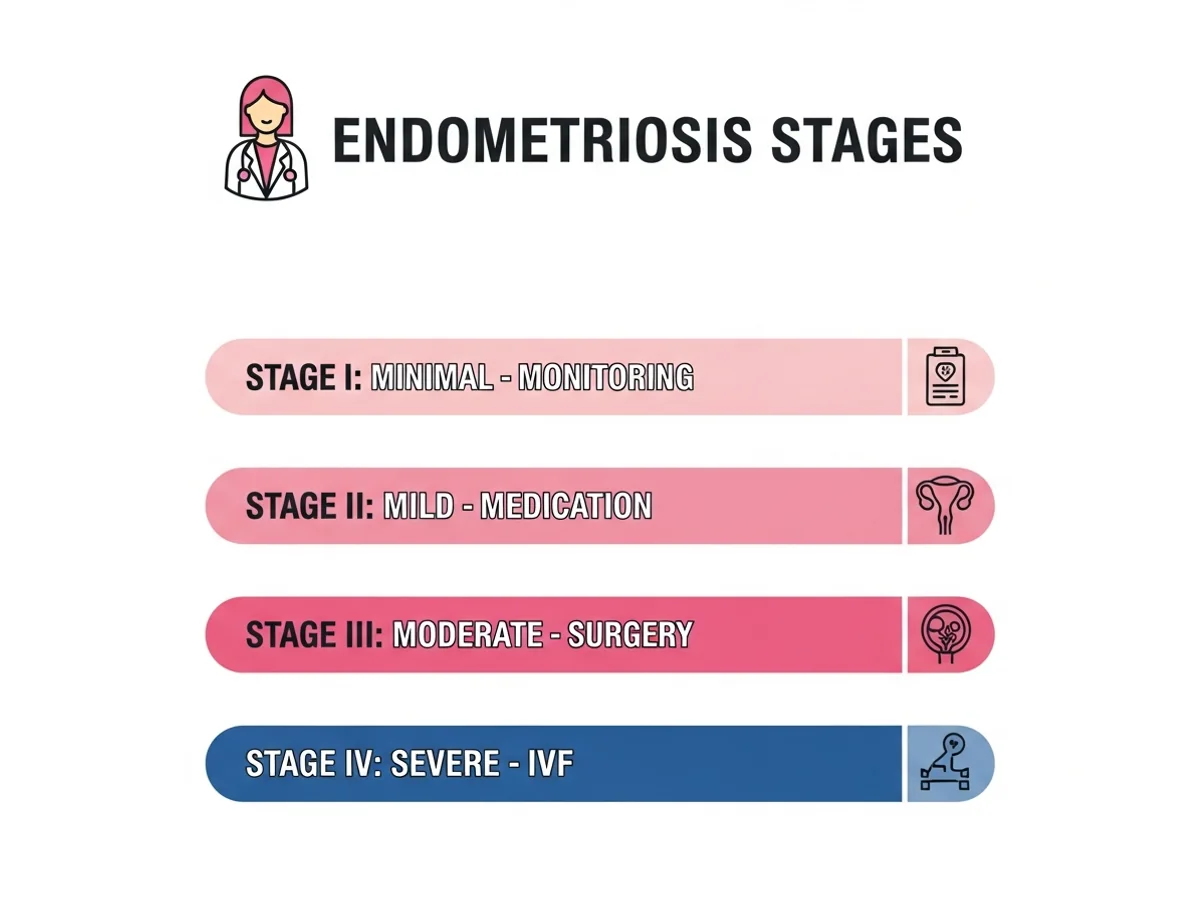
Endometriosis affects an estimated 10 percent of women of reproductive age — roughly 190 million individuals worldwide. Despite its prevalence, the average delay from symptom onset to diagnosis is 7 to 10 years, largely because symptoms like painful periods are often normalized. The condition is classified into four stages by the revised American Society for Reproductive Medicine (rASRM) system: Stage I (minimal), Stage II (mild), Stage III (moderate), and Stage IV (severe). However, the stage does not always correlate with symptom severity — some women with Stage I disease experience debilitating pain, while others with Stage IV may have few symptoms. Endometriosis affects fertility through multiple mechanisms. Endometriotic implants trigger chronic inflammation in the pelvis, producing cytokines and inflammatory mediators that can damage eggs, impair sperm function, and interfere with embryo implantation. Adhesions can distort the anatomy of the fallopian tubes and ovaries, preventing normal egg pickup. Endometriomas — cysts filled with old blood that form on the ovaries — can compress and damage surrounding healthy ovarian tissue, reducing egg reserve over time. Deep infiltrating endometriosis may involve the bowel, bladder, or ureters, requiring specialized surgical management. The encouraging news is that effective treatments exist at every stage. Fertility-preserving laparoscopic surgery, medical suppression therapy, and IVF have all demonstrated strong outcomes for women with endometriosis when the treatment approach is matched to the individual's disease pattern and reproductive goals.
Risk Factors for Endometriosis
Retrograde Menstruation
The most widely accepted theory: menstrual blood flows backward through the fallopian tubes into the pelvic cavity, depositing endometrial cells that implant and grow.
Genetic Predisposition
Women with a first-degree relative (mother or sister) with endometriosis are five to seven times more likely to develop the condition.
Immune System Dysfunction
Impaired immune surveillance may allow displaced endometrial tissue to survive and proliferate outside the uterus instead of being cleared naturally.
Hormonal Factors
Endometriosis is estrogen-dependent. Higher lifetime estrogen exposure — from early menarche, short cycles, or late menopause — increases risk.
Prior Pelvic Surgery
Cesarean section, hysterotomy, or other pelvic surgeries can inadvertently transplant endometrial cells to surgical sites (scar endometriosis).
Mullerian Anomalies
Structural abnormalities of the uterus that obstruct menstrual outflow may promote retrograde menstruation and endometriotic implantation.
Environmental Exposures
Some research links endocrine-disrupting chemicals such as dioxins to an increased risk of developing endometriosis, though the evidence is still evolving.
Inflammatory and Oxidative Stress
Chronic oxidative stress in the pelvic environment may promote the establishment and progression of endometriotic lesions.
How We Diagnose Endometriosis
Transvaginal Ultrasound
High-resolution imaging to detect endometriomas (chocolate cysts) and assess deep infiltrating endometriosis involving the rectovaginal septum or bladder.
Laparoscopy (Gold Standard)
Direct visualization of the pelvis through minimally invasive surgery allows definitive diagnosis, staging, and simultaneous treatment of endometriotic lesions.
CA-125 Blood Test
While not specific enough for diagnosis alone, elevated CA-125 levels in the right clinical context can support suspicion of moderate to severe endometriosis.
Pelvic MRI
Provides detailed mapping of deep infiltrating endometriosis, particularly involving the bowel, ureters, or bladder — essential for surgical planning in complex cases.
Clinical History and Symptom Assessment
A thorough evaluation of pain patterns, menstrual history, and fertility timeline often raises strong clinical suspicion before any imaging is performed.
Fertility-Specific Workup
AMH, antral follicle count, and tubal patency testing assess the reproductive impact of endometriosis and guide whether medical, surgical, or IVF treatment is most appropriate.
Conditions We Treat
How We Treat Endometriosis
Fertility-Preserving Laparoscopic Surgery
Excision or ablation of endometriotic lesions, removal of endometriomas with ovarian tissue conservation, and lysis of adhesions to restore normal pelvic anatomy and improve natural conception chances.
IVF for Endometriosis-Related Infertility
For moderate to severe endometriosis or when surgery alone is insufficient, IVF bypasses the damaged pelvic environment. Dr. Rukkayal's laboratory expertise ensures optimal handling of eggs that may be affected by endometriosis-related inflammation.
Medical Suppression Therapy
Hormonal medications (GnRH agonists or antagonists) to suppress endometriotic growth before or after surgery, or as a pre-IVF preparation to reduce inflammation and improve implantation conditions.
Endometrioma Management
Careful surgical cystectomy that removes the cyst wall while preserving maximum healthy ovarian tissue, maintaining future egg reserve — a critical consideration for women planning pregnancy.
Empirical IUI with Controlled Stimulation
For women with minimal to mild endometriosis, superovulation combined with IUI can improve per-cycle pregnancy rates before proceeding to IVF.
Adenomyosis-Specific Protocols
When endometriosis coexists with adenomyosis, targeted medical preparation of the uterine lining improves implantation receptivity during natural conception or embryo transfer cycles.
Why Choose Dr. Rukkayal?
- Trained in advanced laparoscopic surgery to excise endometriotic lesions while preserving ovarian reserve and fertility potential.
- Direct IVF laboratory involvement means egg and embryo handling accounts for the specific quality challenges associated with endometriosis.
- Comprehensive staging-based approach — treatment intensity is matched to your disease severity and fertility timeline.
- Dual international fellowships (MRCOG UK, FRM Germany) ensure globally validated surgical and reproductive techniques.
- Integrated pain and fertility management — symptom relief and reproductive goals are addressed in parallel, not separately.
- Honest, evidence-based counselling about when surgery helps, when IVF is the better option, and when both are needed.
- Convenient locations across Chennai — Egmore/Chetpet (morning), Mylapore (evening), and Tambaram — plus visiting consultant at Apollo, Motherhood & Cloudnine hospitals.
Your Treatment Journey
Symptom and History Review
Dr. Rukkayal conducts a detailed assessment of your pain patterns, menstrual history, previous treatments, and fertility goals to build an accurate clinical picture.
Imaging and Investigation
Transvaginal ultrasound and, when indicated, MRI provide a non-invasive map of the disease. Blood work evaluates ovarian reserve and inflammatory markers.
Diagnosis and Staging
If laparoscopy is needed, it serves as both a diagnostic and therapeutic procedure — confirming the stage and treating visible disease in the same session.
Individualized Treatment Plan
Based on staging, ovarian reserve, and your personal timeline, Dr. Rukkayal recommends the most effective path — natural conception window post-surgery, IUI, or IVF.
Active Treatment and Monitoring
Whether pursuing natural conception, medicated cycles, or IVF, close monitoring with ultrasound and blood work ensures optimal response and timely adjustments.
Pregnancy Achievement and Ongoing Care
Once pregnant, early monitoring addresses the slightly elevated risks associated with endometriosis. Long-term management guidance is provided for ongoing symptom control.
Have Questions About Your Treatment?
Book a consultation with Dr. Rukkayal Fathima to understand your options and next steps.
Frequently Asked Questions
Many women with mild to moderate endometriosis conceive naturally, especially after surgical treatment restores normal pelvic anatomy. Your chances depend on the stage of disease, your age, ovarian reserve, and whether the tubes are open. Dr. Rukkayal will assess all of these factors to give you a realistic picture.
It depends on the type and extent of disease. Endometriomas larger than 4 cm are often surgically removed before IVF to improve egg retrieval access and reduce inflammation. However, unnecessary surgery on the ovaries can reduce egg reserve. Dr. Rukkayal evaluates each case individually to determine whether surgery, direct IVF, or a combination offers the best outcome.
Chocolate cysts (endometriomas) are ovarian cysts filled with old menstrual blood. Small, asymptomatic endometriomas may be monitored, while larger ones or those interfering with fertility treatment are usually removed surgically. The key is to excise the cyst while preserving as much healthy ovarian tissue as possible.
Research suggests that the inflammatory environment created by endometriosis can negatively affect egg quality and embryo development. This is one reason why Dr. Rukkayal's direct IVF laboratory involvement matters — she can adapt fertilization techniques and culture conditions to optimize outcomes for endometriosis patients.
Adenomyosis involves endometrial tissue growing into the muscular wall of the uterus itself. It can impair implantation and increase miscarriage risk. Treatment typically involves medical suppression to thin the affected uterine tissue before embryo transfer, improving the chances of successful implantation.
The highest natural conception rates after endometriosis surgery occur within the first 6 to 12 months. Dr. Rukkayal will advise you on the optimal window based on your surgical findings and may recommend proceeding directly to IUI or IVF if the disease was extensive.
Yes. Endometriosis has a recurrence rate of approximately 20 to 40 percent within five years after surgery. This is why fertility-focused patients are often counselled to try conceiving promptly after surgical treatment rather than delaying. Pregnancy itself can provide a temporary reprieve from endometriosis progression.
There is no absolute cutoff, but Stage III and IV endometriosis — particularly with bilateral endometriomas, tubal damage, or dense adhesions — significantly reduces natural conception rates. In these cases, IVF is often the most efficient and effective path. Dr. Rukkayal will counsel you based on your specific findings.
Endometriosis can affect IVF outcomes through reduced egg quality, impaired embryo development, and altered endometrial receptivity. However, with appropriate protocols — including pre-treatment suppression therapy when indicated and careful embryo selection — many women with endometriosis achieve successful pregnancies through IVF. Dr. Rukkayal adapts the stimulation protocol based on the stage of your disease.
Related Specialties
Female Infertility Treatment
Comprehensive evaluation of all female infertility causes, including endometriosis and related conditions.
Endoscopy Treatment
Advanced laparoscopic and hysteroscopic procedures for diagnosis and surgical treatment of endometriosis.
IVF Treatment
In vitro fertilization with protocols optimized for endometriosis patients, managed by Dr. Rukkayal's dual clinical-lab expertise.
IUI Treatment
Intrauterine insemination — may be considered for mild endometriosis before proceeding to IVF.
Related Articles
Endometriosis & Fertility: Impact & Options
Understand endometriosis and fertility in Chennai. Learn the impact of endometriosis, stages, diagnosis, and treatment options. Consult Dr. Rukkayal Fathima.
10 min read
Endometriosis Surgery: Fertility Impact
Endometriosis surgery and fertility in Chennai: How it improves your chances of conceiving. Expert insights from Dr. Rukkayal Fathima.
9 min read
Laparoscopy: Is It Needed for Infertility?
Understand the role of laparoscopy for infertility in Chennai. Expert insights on diagnosis, benefits, and when to consider this surgery.
8 min read
Painful Periods & Fertility: What's the Link?
Do painful periods affect fertility? Understand the connection and when to seek help in Chennai. Dr. Rukkayal explains.
9 min read
Ready to Get Started?
Book a consultation with Dr. Rukkayal Fathima about your treatment options
Book AppointmentBook Consultation
Consultation Booked!
Thank you for reaching out. Our team will contact you shortly to confirm your appointment.
Need urgent help? Call us